Checklist for Labeling Compliance in Compounding Pharmacies
Mar 7, 2026

Checklist for Labeling Compliance in Compounding Pharmacies
Proper labeling in 503A and 503B pharmacies is a legal and safety requirement. It helps prevent errors like incorrect dosages, wrong medications, or contamination. Here's what you need to know:
503A Pharmacies: Labels must include patient-specific prescriptions, beyond-use dates (BUDs), and comply with USP standards (e.g., USP <795> for non-sterile and <797> for sterile preparations). Anticipatory compounding is limited to a 30-day supply based on prescription history.
503B Facilities: Labels must state "This is a compounded drug", include batch numbers, expiration dates, facility information, and FDA-required statements like "Not for resale" or "For Office Use Only." MedWatch contact details must also be listed for adverse event reporting.
Failure to meet these standards can lead to FDA warnings, product recalls, or losing regulatory exemptions. Both pharmacy types must maintain accurate records and verify label accuracy to avoid penalties and ensure patient safety.
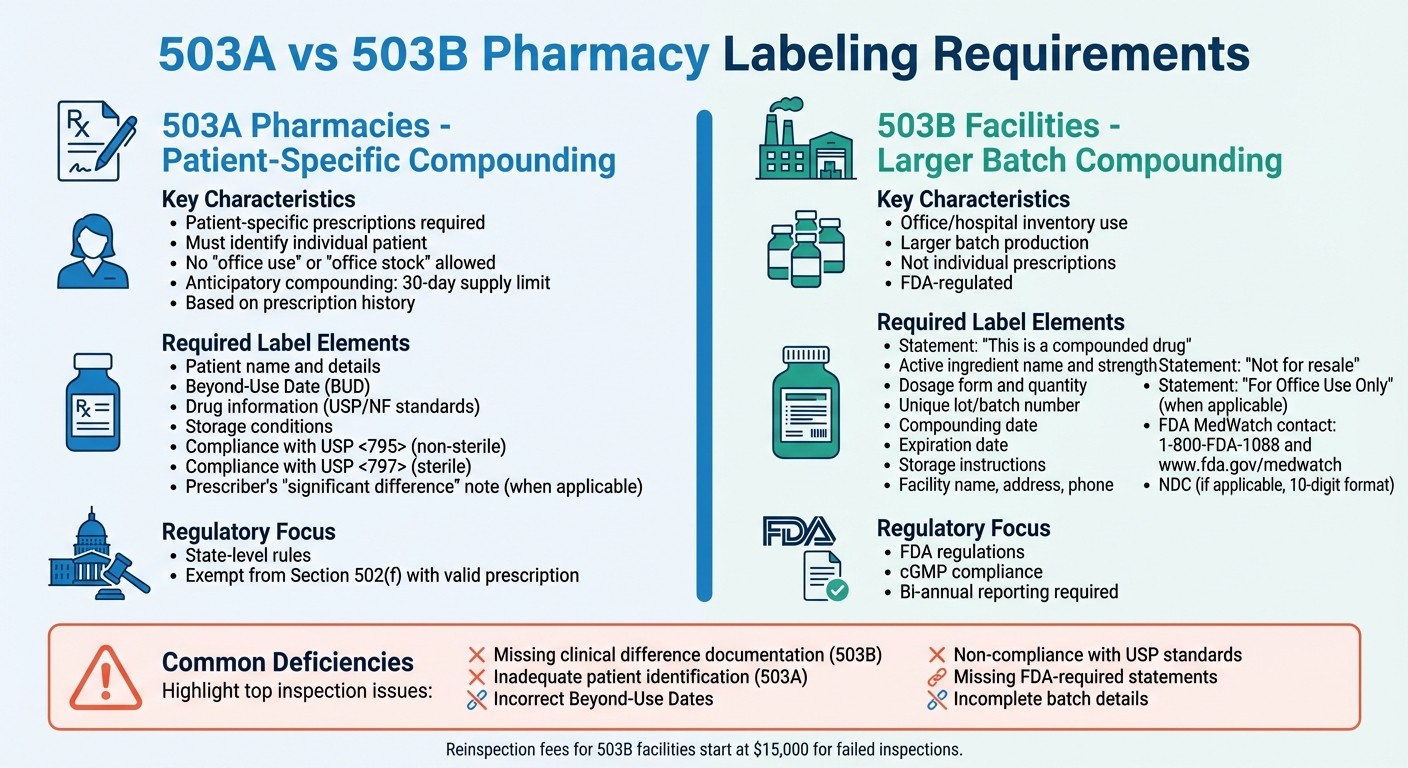
503A vs 503B Pharmacy Labeling Requirements Comparison
cGMP Video Series: 503A and 503B – Similarities and Differences
503A Pharmacy Labeling Checklist
503A pharmacies follow strict guidelines requiring every compounded medication to be tied to a specific patient's prescription. This is what sets them apart from large-scale manufacturing. Each label must align with a valid prescription for an identified patient [4].
Verify Patient-Specific Prescription Details
To comply with 503A standards, every prescription must explicitly identify the patient it’s intended for. Labels cannot be issued for "office use" or "office stock" - these requests don't meet 503A requirements and must be handled by 503B outsourcing facilities instead [4][3].
When compounding an alternative to a commercial drug, the prescription must include a prescriber's note explaining the "significant difference" for the patient. For instance, a prescriber might specify "No Dye X, patient allergy" to justify why the compounded medication is necessary [3][2].
For anticipatory compounding - preparing medications before receiving a prescription - limit production to the highest 30-day supply based on past prescription history. This is only allowed if there is an established relationship with the prescriber or patient and a consistent record of valid prescriptions [4].
Include Drug Information and Beyond-Use Date (BUD)
All bulk drug substances used must meet USP/NF monograph standards or be FDA-approved. Additionally, they must come with a valid certificate of analysis from an FDA-registered source [3]. Beyond-use dates and storage conditions should follow USP <795> for nonsterile preparations and USP <797> for sterile ones [3][7].
Ensure USP Compliance and Exemptions
Once the drug details are confirmed, ensure compliance with all relevant USP standards. 503A pharmacies are exempt from Section 502(f) of the FD&C Act, which mandates "adequate directions for use", as long as the medication is compounded for a specific patient based on a valid prescription [4][3].
"The prescription requirement under section 503A is a critical mechanism to distinguish compounding by a licensed pharmacist or licensed physician from conventional manufacturing." - FDA Guidance for Industry [4]
This focus on patient-specific prescriptions is essential to maintaining 503A status and the associated regulatory exemptions.
503B Pharmacy Labeling Checklist
503B outsourcing facilities are responsible for compounding drugs in larger batches, intended for use in offices, hospital inventories, and clinics - not for individual prescriptions. Because of this, their labels must meet FDA regulations, rather than just adhering to state-level rules [5].
Label Identification and Drug Information
Every label from a 503B facility must include the statement: "This is a compounded drug" [5]. This ensures that healthcare providers and patients are aware they are using a compounded product, not an FDA-approved commercial medication.
The label must also provide the established name of the active ingredient, its strength per unit dose, the dosage form (e.g., vial, syringe, or tablet), and the quantity or volume in the packaging [9]. If the product has a National Drug Code (NDC), it should be displayed in the standard 10-digit format with dashes [9].
Batch Details and Facility Information
Batch tracking is a critical component for 503B operations. Labels must include a unique lot or batch number to link the product to its production records [1]. Additionally, the label should display the compounding date, expiration date (based on stability studies), and any specific storage instructions, such as temperature requirements [1].
The facility's name, address, and phone number must also appear on the label [1]. Lori Cantin, Acting Branch Chief at the FDA, emphasizes the importance of this:
"Outsourcing facility drug product labels [must] clearly identify the outsourcing facility as the producer of the drug product" [1].
If a building houses both a 503A and a 503B facility, labels must clearly indicate which entity produced the drug [5].
Required Statements and Reporting Information
503B facilities are prohibited from selling to entities that will resell the drug. To comply, labels must include the statement: "Not for resale" [8]. For products designated for office stock rather than direct patient use, the label should also state: "For Office Use Only" [8].
Adverse event reporting information is another essential element. Labels must display the FDA MedWatch phone number and website, allowing for quick reporting of any unexpected reactions [1]. Furthermore, 503B facilities are required to report serious adverse drug experiences to the FDA within 15 calendar days, and these reports must include a copy of the current label [1].
Core Label Element | FDA Requirement Details |
|---|---|
Compounding Status | Statement: "This is a compounded drug" |
Active Ingredients | Full chemical name, strength, and quantity |
Beyond-Use Date | Expiration timeline based on stability studies |
Storage | Specific temperature and environmental instructions |
Facility Info | Name, address, and phone number of the 503B facility |
Lot/Batch Number | Unique identifier for production tracking |
MedWatch Info | FDA MedWatch phone number and website for reporting |
Resale Status | Statement: "Not for resale" |
These labeling standards ensure compliance, transparency, and safety, laying a solid foundation for thorough verification and record-keeping in later stages.
Verification and Documentation Procedures
After establishing labeling standards, the next critical step is implementing strong verification and documentation practices. These processes are essential not just for regulatory compliance but also for ensuring patient safety. While creating accurate labels is crucial, verifying their accuracy and maintaining thorough records are equally important, especially during inspections. Both 503A and 503B facilities must have structured procedures to identify and correct errors before products leave the facility. This verification step complements the labeling protocols discussed earlier, ensuring compliance with all regulations.
Review and Cross-Check Label Information
Before dispensing, labels must be carefully reviewed against their source documents. For 503B facilities, this involves comparing labels to master or batch production records. According to 21 CFR § 211.125:
"Labeling materials issued for a batch shall be carefully examined for identity and conformity to the labeling specified in the master or batch production records" [10].
Facilities should document the total number of labels issued, used, and returned, and investigate any discrepancies that exceed predefined limits [10]. If reconciliation is waived for cut or roll labeling, a 100% physical inspection is required to ensure every unit has the correct label [10].
For 503B products, it’s also necessary to verify that each order includes the prescriber’s clinical difference determination. If this information is missing, document the prescriber’s contact details and the outcome of the inquiry [2]. Meanwhile, 503A pharmacies should ensure that anticipatory compounding quantities align with a 30-day supply based on historical prescription data [4].
Once labels are confirmed, proper documentation ensures readiness for audits and inspections.
Maintain Records
Accurate and detailed documentation is essential for demonstrating compliance during inspections. For 503A pharmacies, records should include patient-specific prescriptions and production logs to verify that anticipatory compounding stays within the 30-day supply limit [4]. For 503B facilities, it’s important to maintain records of prescriber determinations for clinical differences. These records should include specific notations, such as "Liquid form, patient can't swallow tablet" or "No Dye X, patient allergy" [2].
Facilities should also establish written labeling control procedures, securely store returned labels to prevent mix-ups, and destroy excess labels with specific lot numbers [10]. These practices help ensure compliance and provide a solid defense during FDA inspections, which often involve an in-depth review of operational records [6].
Documentation Type | Pharmacy Type | Essential Requirement |
|---|---|---|
Patient-Specific Prescription | 503A | Must identify the individual patient before the drug leaves the facility [4] |
Anticipatory Production Log | 503A | Must prove "limited quantities" based on a 30-day historical supply [4] |
Clinical Difference Statement | 503B | Must specify the change and the clinical reason for that change for the patient [2] |
Prescriber Contact Log | 503B | Must include date, name of contact, and clinical determination if not on the original order [2] |
Common Deficiencies and Inspection Focus Areas
Regulatory inspections often zero in on specific labeling issues that could compromise patient safety or fail to meet compliance standards.
Identify Common Labeling Errors
One of the most frequent 503B deficiencies is missing clinical difference documentation. When compounding a drug that's effectively a copy of an FDA-approved product, the prescriber must clearly document the clinical difference. For instance:
"If a prescription or order identifies only a patient name and product formulation, this would not be sufficient to establish that the determination [of clinical difference] described by section 503B(d)8 has been made." [2]
This documentation must detail both the change and the clinical reason, such as "Liquid form, patient can't swallow tablet" or "No Dye X, patient allergy" [2].
For 503A pharmacies, inadequate patient identification is a common issue. Prescriptions written for "office use" or addressed to the prescriber rather than a specific patient fail to meet 503A requirements [4].
Another frequent problem is incorrect Beyond-Use Dates (BUDs). Facilities often assign BUDs without proper stability data to back them up [11]. This can lead to real risks, such as products losing potency or becoming contaminated before their expiration date. BUDs must be based on specific stability studies, not on generic estimates [11].
Inspectors also frequently find non-compliance with USP standards in 503A pharmacies. Common citations include failures to meet USP <795> (non-sterile) and USP <797> (sterile) guidelines [11]. In 503B facilities, violations often stem from missing FDA-required statements, incomplete batch details, or absent facility information [11]. Additionally, 503B facilities are required to electronically report all compounded drugs from the previous six months, including active ingredients, dosage forms, and routes of administration. Failing to do so is another common citation [12].
The 2012 tragedy at the New England Compounding Center, where fake prescriptions were used to hide bulk manufacturing, led to the creation of the 503B category for stricter oversight [12]. Addressing these errors is essential to avoid regulatory penalties.
Prepare for Regulatory Inspections
To prepare for inspections, facilities must address these common errors and focus on compliance. Inspectors will closely examine labeling details. For 503B container labels, they will check for the inclusion of MedWatch contact information (www.fda.gov/medwatch and 1-800-FDA-1088) [13]. They will also verify that drugs labeled "For office use only" have proper patient-specific prescriptions, as incorrect designations can nullify 503B exemptions.
Label quality is another critical area. Inspectors look for issues like bubbling labels, missing "Rx only" symbols, or mismatched lot numbers and expiration dates between inner and outer containers [14]. These flaws can indicate non-compliance.
Conducting mock audits can help ensure your documentation systems and staff are prepared for FDA and state board inspections [15]:
"Compliance is not a checklist; it is a system." [15]
If you're a 503A pharmacy sourcing from 503B facilities, you share liability. Always vet your suppliers by checking the FDA website for current registration, pending 483 violations, or recent recalls [8]. Also, monitor the FDA shortage list closely - 503B facilities can only compound "essentially a copy" of a drug while it remains on this list, with a 60-day grace period after removal [8].
Failed inspections can have serious financial and operational consequences. For instance, 503B outsourcing facilities face reinspection fees starting at $15,000 (adjusted for inflation) if they fail an initial inspection [12]. Beyond the monetary impact, deficiencies can lead to warning letters, product recalls, and restrictions on operations. Proactive preparation is key to protecting both your facility and your patients.
Deficiency Type | 503A Impact | 503B Impact |
|---|---|---|
Missing Clinical Difference | Not applicable | Invalidates exemption for "essentially a copy" drugs [2] |
Inadequate Patient ID | Violates 503A prescription requirement [4] | May invalidate "office use" labeling |
Incorrect BUD | Fails USP <795>/<797> compliance [11] | Fails cGMP stability requirements [11] |
Missing MedWatch Info | Not federally mandated | Mandatory on all container labels [13] |
Incomplete Drug Reporting | Not applicable | Violates bi-annual reporting requirement [12] |
Conclusion
Summary of Labeling Best Practices
Ensuring proper labeling compliance is critical for protecting patients and maintaining your facility's legal standing. For 503A facilities, labels must meet USP standards and include patient-specific information, while 503B labels require the compounded drug statement, detailed batch information, and clear facility identification[5][2]. Following these guidelines not only prioritizes patient safety but also shields your facility from potential regulatory issues.
The line between 503A and 503B facilities is important. The prescription requirement differentiates compounding by licensed professionals from traditional manufacturing[4]. This distinction ensures compounded drugs are tailored to genuine patient needs rather than being misused as unapproved manufacturing.
Why Consistent Compliance Matters
Labeling mistakes can lead to serious consequences, both for patients and your facility. Accurate labeling - covering everything from patient details to batch numbers - is crucial. There have been cases where patients were hospitalized due to compounded drugs with incorrect strengths[4]. In one tragic event, a fungal meningitis outbreak caused by contaminated injectable drugs resulted in 64 deaths and 793 infections[4]. These incidents highlight the life-or-death importance of precise labeling.
Beyond patient safety, proper labeling helps maintain critical regulatory exemptions. Both 503A and 503B facilities benefit from conditional exemptions under FDA rules, such as premarket approval (Section 505) and "adequate directions for use" labeling (Section 502(f)(6))[2][4]. Noncompliance can put these exemptions at risk, leading to enforcement actions, warning letters, and costly reinspection fees - starting at $15,000 for 503B facilities[12].
Staying compliant also ensures smoother operations by keeping your facility prepared for inspections and avoiding setbacks like failed inspections or recalls. Most importantly, strong labeling practices foster trust among prescribers, patients, and regulators, proving that safety and quality are always at the forefront of your compounding process.
FAQs
What are the main differences in labeling requirements for 503A and 503B pharmacies?
The labeling requirements for 503A and 503B pharmacies vary significantly because of their different roles and regulatory expectations.
503A pharmacies, which specialize in patient-specific compounding, must include essential details on their labels. These typically consist of the patient’s name, the drug name, strength, dosage form, route of administration, and the Beyond-Use Date (BUD). These requirements align with guidelines from USP <795> and <797>, as well as individual state board regulations.
Meanwhile, 503B outsourcing facilities, which produce medications in larger batches for office use, are held to stricter labeling standards under CGMP regulations. Their labels must provide more detailed information, including the product name, strength, dosage form, lot or batch number, expiration date, storage instructions, necessary warnings, and a statement confirming the product was compounded in an FDA-registered outsourcing facility. These detailed labels also play a critical role in traceability and recall efforts, reflecting the heightened regulatory oversight for 503B facilities.
In short, labeling for 503A pharmacies is patient-specific and straightforward, while 503B labels are comprehensive and designed for broader distribution, ensuring compliance with rigorous CGMP standards.
Why must 503B facilities include FDA MedWatch information on their labels?
Including FDA MedWatch details on labels plays a key role in meeting the required standards for adverse-event reporting. This information gives both patients and healthcare providers a straightforward way to report potential side effects directly to the FDA, supporting efforts to monitor product safety and safeguard public health.
For 503B outsourcing facilities, adding this information highlights their dedication to openness, adherence to regulations, and prioritization of patient safety - cornerstones of their operational framework.
What steps should 503A pharmacies take to comply with anticipatory compounding limits?
To stay compliant, 503A pharmacies must restrict anticipatory compounding to what is permitted under FDA regulations, ensuring every preparation is tied to a valid prescription or prescriber authorization. Always apply the most cautious beyond-use dates (BUDs), referring to USP <795> for non-sterile preparations and USP <797> for sterile ones. It's also crucial to follow strict labeling requirements and align with the FDA's guidance on 503A compounding practices to uphold regulatory standards.
Download Now